Patient selection criteria
Cochlear implantation is mainly used for the treatment of severe or very severe sensorineural hearing loss in both ears.
1. Selection criteria for prelingual deaf patients:
① The implantation age is usually 12 months to 6 years. The smaller the implantation age, the better the effect, but it is necessary to prevent complications such as accidental anesthesia, excessive blood loss, and damage to the inner and outer nerves of the temporal bone. Implantation of cochlear implants is not currently recommended for children younger than 6 months. However, deafness caused by meningitis is at risk of cochlear ossification. It is recommended that surgery be performed as soon as possible under conditions of complete surgery. Children or adolescents over 6 years of age need a certain listening and speaking foundation.
②Severe or very severe sensorineural hearing loss in both ears. After comprehensive audiological evaluation, children with severe hearing loss who wear hearing aids for 3 to 6 months are not effective or have unsatisfactory results. Cochlear implantation should be performed; children with severe hearing loss can consider direct cochlear implantation.
③ There are no contraindications for surgery.
④ The guardian and / or the implanter have a correct understanding and appropriate expectations of the cochlear implant.
⑤ Have the conditions for hearing and speech rehabilitation education.
2. Selection criteria for post-speech deaf patients:
① Post-speech deaf patients of all ages.
② Severe or extremely severe sensorineural hearing loss in both ears cannot rely on hearing aids for normal auditory speech communication.
③ There are no contraindications for surgery.
④ The implanter and / or the guardian have a correct understanding and appropriate expectations of the cochlear implant.
Contraindications to surgery
1. Absolute contraindications: severe malformation of the inner ear, such as Michel malformation; absence or disruption of the auditory nerve; acute purulent inflammation in the middle ear mastoid process
2. Relative contraindications: frequent seizures cannot be controlled; severe mental, intellectual, behavioral, and psychological disorders cannot be combined with auditory speech training.
Excerpt: Cochlear Implant Working Guide (2013)
Minimally invasive cochlear implant surgery
Cochlear implantation of small incisions, cochlear implantation of 2.5-4.0cm small incisions have proven effective, small incisions have been proven to reduce bleeding, shorten the operation time, and basically eliminate the risk of flap necrosis Complications of surgery in young children are of great significance.
Excerpt from: Dai Pu: Some considerations of minimally invasive cochlear implant surgery, Proceedings of the 14th Military Academy of Otolaryngology Head and Neck Surgery
Cochlear Surgery Nursing
Preoperative and postoperative care
Preoperative care
1.1 Psychological Nursing
After the patient is admitted to the hospital, parents or family members need to help them become familiar with the environment (especially children) as soon as possible, and eliminate the fear of the hospital environment.
1.2 Preoperative preparation
Assist doctors to complete various pre-operative examinations of patients; cochlear implantation is a general anesthesia operation. Food and water are forbidden 8 to 12 hours before operation to avoid the risk of aspiration when anesthesia is intubated.
1.3 Preoperative skin preparation
The skin preparation range is 3 ~ 5cm behind the ear, and you can shave your head. After skin preparation, the patient should be instructed to take a bath, especially in children. The cut hair will cause harm to immature skin and need to be cleaned in time.
1.4 Parent Expectation
Before surgery, we must fully understand the benefits and deficiencies of cochlear implants, and we must have appropriate expectations to achieve satisfactory results.
2. Postoperative care
2.1 Nursing after general anesthesia
The supine side should be taken after the operation (both sides are implanted simultaneously and the supine position is used), with the ears facing upwards. Crying and restlessness often occur when the child is awake at the beginning of general anesthesia. Care should be taken to protect the child's safety and prevent falling from bed.
You can eat warm, digestible liquid or semi-liquid diets 4 to 6 hours after surgery, and eat water prematurely. When the child is distressed, it may easily cause the risk of aspiration or asphyxiation.
3. Postoperative guidance
3.1 startup and commissioning
Start up about 1 month after the operation, and arrange the next debugging according to the instructions of the audiologist.
3.2 Postoperative speech rehabilitation training
For children, parents need to send them to professional hearing and speech rehabilitation institutions for rehabilitation training. Language training requires the cooperation of parents. Don't let children see oral pronunciation, sign language, etc. Use oral communication as the first choice.
3.3 Correct use and maintenance of cochlear implants after surgery
Avoid local violent collision and compression, avoid humidity and rain, and prevent external force damage caused by rough operation.
Excerpt: Feng Xiulan, Yuan Chen, Wang Lin'e *, Analysis of perioperative nursing experience in children with cochlear implants. Chinese Journal of Hearing, Speech and Rehabilitation Science, 2009, Issue 5, 73-76
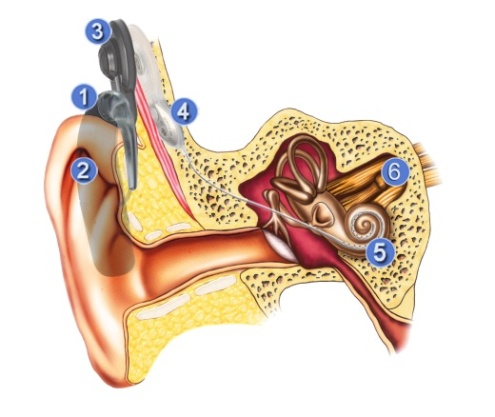
Cochlear implant working principle:
1. Microphone to collect sound
2. Speech processor processes, encodes and digitizes the collected sound
3. The compiled code is transmitted to the body through the transmission coil
4. The receiving stimulator decodes the received signal and converts it into a special electrical signal that is transmitted to the electrodes in the cochlea via a wire.
5. Intracochlear electrodes stimulate different parts of the cochlea according to the frequency of incoming sound
6. The auditory nerve produces nerve impulses and passes to the auditory center of the brain to produce hearing
Cochlear implant (CI) is the standard of medical care for treating bilaterally severe to very severe sensorineural deaf children and adults. Because the ultimate and ongoing goal of cochlear implants is to improve the hearing performance of hearing impaired patients, bilateral cochlear implants are also a potential approach. Potential benefits on both sides include the binaural sum effect, squelch effect, the equivalent head shadow effect on each ear, improved hearing under noise, sound localization ability, and spatial effects of masking release; potential disadvantages include additional or extended surgery, Unproven cost / benefit situation and loss of ability to use future technologies or drugs to treat cochlear implants [1].
Children's bilateral cochlear implantation: Experimental results show that the child's recognition rate reaches 100% in both tone recognition and bisyllable word recognition. In terms of vowels, both sides are slightly better than one side. In terms of initial recognition and short sentence recognition, the speech recognition rate of bilateral cochlear implants is much higher than that of unilateral. In daily life, children wear bilateral cochlear implants more than unilateral speech recognition rates. Hearing orientation should be good [2].
Successive bilateral cochlear implantation in adolescents: Studies have shown that adolescent implanters who have successively received bilateral cochlear implants report a significant improvement in hearing after a second cochlear implant (CI2).
Speech discrimination ability of bilateral cochlear implanters in noisy environment: Research shows that under different signal-to-noise ratios (signal-to-noise ratios of 0, -5, -10, and -15), the unilateral cochlear The average discrimination ability is close to 0%, and the average scores of bilateral cochlear implants are 80%, 72%, 68%, and 54%. Patients with bilateral cochlear implants have a clear advantage [4].
Conclusion: Bilateral cochlear implants improve the speech recognition rate of patients [2].
references:
1. Wanna G B, Gifford R H, Mcrackan T R, et al. Bilateral cochlear implantation. [J] .Otolaryngologic Clinics of North America, 2012, 45 (1): 81.
2.Liu Qiaoyun, Huang Zhaoming, Sun Xibin, et al. A case study of the effects of bilateral cochlear implantation on hearing recognition in children [J]. Chinese Journal of Hearing and Speech Rehabilitation Science, 2008 (1): 51-53.
3. Feiedmann D R, Green J, Fang Y, et al. Sequential bilateral cochlear implantation in the adolescent population [J]. Laryngoscope, 2015,125 (8): 1952-8.
4. Qu Jianguo, Jin Hao, Xu You, et al. Speech discrimination ability of bilateral cochlear implants under noise environment [J]. Chinese Journal of Otorhinolaryngology Head and Neck Surgery, 2001,36 (6): 433-435.
Abstract: Senile deafness is the most common hearing impairment in humans. It is manifested as a degenerative disease that is closely related to the aging process and involves the outer ear, middle ear, inner ear, central auditory pathway and cortical cognition.
Causes of senile deafness:
1. The irreversible aging process of the body.
2. Genetic factors: The age of onset of senile deafness can range from more than 30 to more than 80 years. The speed of the process also varies from person to person, and is familial and regional. It is affected by genetic factors.
3. The impact of environmental and individual factors: such as the cumulative effect of various noise damages, the accumulation of ototoxic effects of drugs or chemical agents, etc.
Symptoms of senile deafness:
1. Complain that you can hear but cannot understand the words.
2. Senile deafness, mainly cochlear lesions, has a revival phenomenon, manifested as being inaudible in a low voice, and loud and loud, and the dynamic range of the frequency response is limited when a hearing aid is selected.
3. Difficult to distinguish sound in noisy environment and affect communication.
4. It is difficult to identify the position of the sound source.
5. Often accompanied by high frequency tinnitus.
Treatment of senile deafness:
1. For patients with severe hearing loss, you can choose cochlear implantation. A recent study [1] shows that cochlear implantation in the elderly is not affected by age, but the general condition of the elderly is an important consideration for surgical decision-making and perioperative period.
Supplementary information: In many older people, age-related hearing loss is often not a concern, so hearing loss is often considered an unfortunate but insignificant component of aging. Researchers have reported that hearing loss may accelerate age-related cognitive decline, and more effective interventions in hearing loss may help delay cognitive decline and dementia [2].
Excerpt: Xie Jing, Gong Shusheng. Senile deafness [J]. Chinese Journal of General Practitioners, 2013 (6): 416-418.
References:
1. Leung J, Wang NY, Yeagle JD, et al. Predictive models cochlear implantation in elderly candidates. Arch Otolaryngol Head Neck Surg, 2005, 131: 1049-1054.
2. Peracino A. Hearing loss and dementia in the aging population. [J]. Audiology & neuro-otology, 2014, 19 Suppl 1 (1): 6-9.
Cases where there is a gap in hearing between the two ears are collectively referred to as Asymmetric Hearing Loss (AHL), which refers to a certain degree of asymmetry in the hearing sensitivity of the ears. An extreme example is that the poor ear is fully deaf and the contralateral ear has normal hearing. Or only mild hearing loss. This extreme example is generally referred to as Unilateral Hearing Loss (UHL) or Single Sided Deafness (SSD). At this time, the frequency of 4 frequencies (ie, 0.5, 1, 2 and 4 kHz) between the ears The asymmetry difference of the pure tone threshold is 30dBHL or more, and at the same time, the poor ear hearing reaches the traditional cochlear implantation standard. Another well-recognized additional condition of UHL is that the average threshold of good ears should be better than 60 dBHL, which makes it clear that it is not suitable to implant cochlear implants on the side of good ears [1].
Based on comprehensive neonatal hearing screening data, the incidence of unilateral deaf children is 1-3% [1] The incidence of unilateral deafness is high in adults, especially in the elderly can be as high as 18% [2]
Causes of unilateral deafness: The causes of unilateral deafness can be hereditary, congenital, and acquired, such as unilateral cochlear nerve dysplasia (Cochlear Nerve Deficiency CND), congenital microtia, large vestibular aqueduct syndrome, Auditory neuropathy, viral / bacterial infectious deafness, unilateral sudden deafness, noise-induced deafness, Meniere's disease, head trauma, unilateral auditory neuroma, etc. [3,4].
Harm of unilateral deafness: Asymmetric hearing loss and speech recognition rate of patients with unilateral deafness will decrease [5], but generally will not seriously affect the speech and language development of patients, and the academic performance of some patients is not directly affected. Patients with lateral hearing loss have not received any intervention throughout their lives [6].
Intervention for unilateral hearing loss: Interventions are recommended for asymmetric hearing loss and unilateral hearing loss. Binaural listening can identify the source of the sound, which can help implanters quickly identify and locate the talker during group communication. Because of unilateral deafness or unilateral cochlear implantation, the speaker's speech cues, such as tones, are weak, so binaural listening is particularly important [7,8].
Chart:
Table 1. Definition of SSD and AHL based on pure tone average hearing threshold [9]
|
SSD
|
Poorear
|
Tosevere hearing loss
|
|
Goodear
|
≤30dB HL
including 4000 Hz
|
|
AHL
|
Poor ear
|
To severe hearing loss
|
|
Good ear
|
≥30dB HL including 4000 Hz
|
|
≤60dB HL including 4000 Hz
|
|
Hearingasymmetry of both ears
|
≥30dB HL(poorear PTA4-good ear PTA4))
|
|
PTA4 = Four-frequency pure tone averagethreshold
|
References:
1. Christophe Vincent, Susan Arndt, Jill B. Firszt, Bernard Fraysse, Pádraig T. Kitterick, Blake C. Papsin, Ad Snik, Paul Van de Heyning, Olivier Deguine, Mathieu Marx: Identification and Evaluation of Co- chlear Implant Candidates with Asymmetrical Hearing Loss. Audiol Neurotol 2015; 20 (suppl 1).
2. Agrawal Y1, Platz EA, Niparko JK: Prevalence of hearing loss and differences by demographic characteristics among US adults: data from the National Health and Nutrition Examination Survey, 1999- 2004. Arch Intern Med. 2008 Jul 28; 168 (14) : 1522-1530.
3. Tharpe AM1, Sladen DP: Causation of permanent unilateral and mild bilateral hearing loss in children. Trends Amplif. 2008 Mar; 12 (1): 17-25.
4. Susan Arndt, Susanne Prosse, Roland Laszig, Thomas Wesarg, Antje Aschendorff, Frederike Hassepass: Cochlear Implantation in Children with Single-Sided Deafness: Does Aetiology and Duration of Deafness Matter Audiol Neurotol 2015; 20 (suppl 1): 21–30 .
5. Lieu JE1, Tye-Murray N, Karzon RK, Piccirillo JF: Unilateral hearing loss is associated with worse speech-language scores in children. Pediatrics. 2010 Jun; 125 (6): e1348-1355.
6. Weaver, J: Single-Sided Deafness: Causes, and Solutions, Take many Forms. Hearing Journal. (2015) 68 (3): p. 22-24.
7. 19.Kerber, S. and B.U. Seeber: Sound localization in noise by normal-hearing listeners and cochlear implant users. Ear Hear. 2012, 33 (4): p. 445-457.
8. 20.Loizou, P.C. Speech processing in vocoder-centric cochlear implants. Adv Otorhinolaryngol. 2006, 64: p. 109-143.
9. Vincent C, Arndt S, Firszt J B, et al. Identification and Evaluation of Cochlear Implant Candidates with Asymmetrical Hearing Loss [J]. Audiol- ogy & Neurotology, 2015, 20 Suppl 1: 87-89
[LiteratureExpress] Analysis of the rehabilitation effect of 74 cases of children withprelingual deafness after Nurotron cochlear implantation
Author:Zengxian Hai, Zhao Peng,Wang Peng, Yang Tingjun, Qiushu Qi, Zhao Hailiang
【Key words】
Prelingualdeafness; Chinese production; Cochlear implant; Rehabilitation
【Purpose】
Toevaluate the rehabilitation effect of Nurotron cochlear implantation inprelingually deaf children.
【Method】
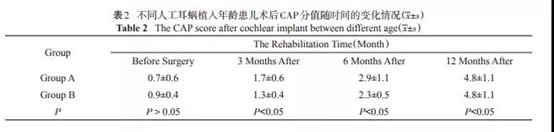
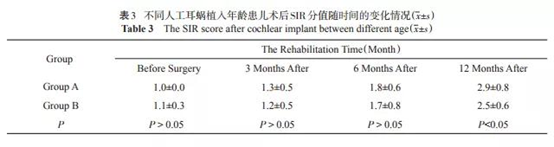
Atotal of 74 children with severe or extremely severe sensorineural deafness whounderwent unilateral Nurotron cochlear implantation at the OtolaryngologyHospital of Longgang District, Shenzhen from June 2012 to December 2016 wereselected as the research subjects. According to the cochlear implants when ageis divided into group A (1-6 years old) and group B (7-14), application ofauditory behavior classification standard, classification standard speechintelligibility and acoustic field words frequency hearing threshold for allchildren in preoperative and postoperative 3 months, 6 months after operation,postoperative 12 months auditory verbal ability assessment.
【Result】
At3, 6, and 12 months after cochlear implantation, the rehabilitation effect ofthe two groups of children gradually improved with the extension of therehabilitation time. Among them, the rehabilitation effect of the group A wasbetter than that of the group B.
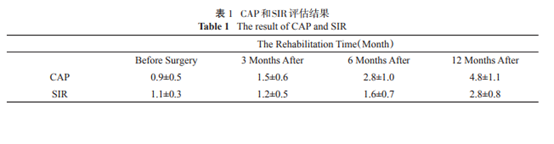
Withthe extension of rehabilitation time, the children's auditory behavior ratingscale (CAP) and speech intelligibility rating scale (SIR) scores have graduallyincreased, see Table 1-3:
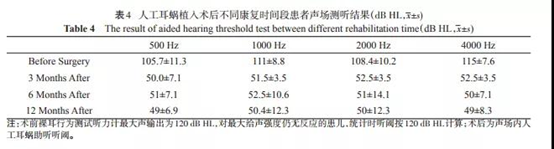
The auditory threshold of speech frequency in the two groups wassignificantly improved 3 months after the operation compared with that before.There was no significant difference in the auditory threshold of the acousticfield speech frequency at 3, 6 and 12 months after the operation, as shown intable 4:
【 Conclusion 】
The Nurotron cochlear implant can significantly improve thehearing and speech ability of children with severe or extremely severe sensorineuralhearing loss. With the extension of rehabilitation time, the hearing and speechability of children with Prelingualdeafness gradually improves. The rehabilitation time and the age at thetime of cochlear implantation are important factors affecting the effect ofhearing and speech rehabilitation of children with Prelingual deafness.
【 Discussion 】
Research has shown that the younger the age of cochlearimplantation, the steeper the auditory development curve, the faster the speedof postoperative hearing rehabilitation, on the contrary, the hearing curve isflat, and the hearing rehabilitation effect is slower. This study shows thatfor children with Chinese brand cochlear implants, the CAP and SIR scores ofthe two groups of children gradually increase with the postoperative languagerehabilitation learning, and the CAP and SIR of the 1-6 year old group aresignificantly higher than 7-14 The age group indicates that the implantation ofChinese brand cochlear implants is very helpful to the hearing and speechability of deaf children, and that early cochlear implantation can benefitchildren more.
This study shows that the hearing threshold reaches a relativelyideal state within 3 months after operation, and remains stable within one yearafter operation. Based on the analysis of hearing and speech rehabilitationability of Nurotron cochlear implantation in China and the evaluation ofhearing aid threshold, we can initially conclude that Nurotron cochlear implanthas good stability and effectiveness.
This article was published in Chinese Journal of Otology 2018 Vol. 16 No. 3 P344-347


